Arthroscopic surgery is routine and now the state of the art for equine joint surgery. It is minimally invasive and therefore much more gently for the joint.
After inserting a needle into the joint cavity which is then distended with sterile isotonic polyionic Ringer’s solution or gas the arthroscope (optic) is positioned through a small (1cm) incision. With the help of the optic the joint surface can be seen on a monitor. Hand instruments like probes, forceps, rongeurs and cannulas are introduced through a second portal.
Indications for arthroscopy can be of diagnostic or surgical reason. In case of more complicated medical findings diagnostic arthroscopy can provide detailed information about the joint surface, treating options and prognosis. Treating options include fragment removal, debridement of cartilage lesions and joint lavage. In the stifle loose tissue of the injured cranial ligament and/or the meniscus (meniscal tears) can be arthroscopically debrided with a motorised synovial receptor. In case of a synovial infection arthroscopic lavage and/or removal of foreign bodies or posttraumatic fragments is inevitable. Septic arthritis is a common consequence of bacteremia and septicemia in foals. In these cases arthroscopy has several advantages over simple needle lavage leading to a much better prognosis. It allows thorough debridement, removal of fibrin and lavage of all compartment as well as evaluation and debridement of cartilage lesions.
If OCD (Osteochondrosis dissecans) results in synovitis or joint inflammation with the clinical signs of pain and lameness surgical debridement of the lesion is the treatment of choice. Reasons for arthroscopy in the coffin, pastern, fetlock, carpal or tarsocrural joint are mainly OCD fragments on the dorsal or palmar/plantar aspect.
Due to an increasing standard of quality claim in horse marketing prophylactic surgery is justified if vigorous athletic activity is planned.
Beside OCD lesions subchondral cyst-like lesions may occur at many locations in the horse. Treatment involves either steroid injection into the cyst lining, with or without surgery, and arthroscopic extirpation. The most common region for subchondral cystic lesions is the stifle joint, followed by the fetlock, elbow and shoulder joint.
Another indication for endoscopic surgery are affected tendons, especially flexor tendons, and their related structures inside a sheath situated at the level of great motion joints where they permit a better gliding function (digital flexor tendon sheath, carpal sheath, tarsal sheath). Many abnormalities can be visualized and treated as debridement of fibrillated and torn areas of the tendons, synovial mass and adhesion removal as well as desmotomy.
In cases of pain localized in the navicular region or an infected podotrochlear bursa due to a foreign body navicular bursoscopy has developed a diagnostic and therapeutic tool.
-

- arthroscopy
-

- OCD (Chip)
-
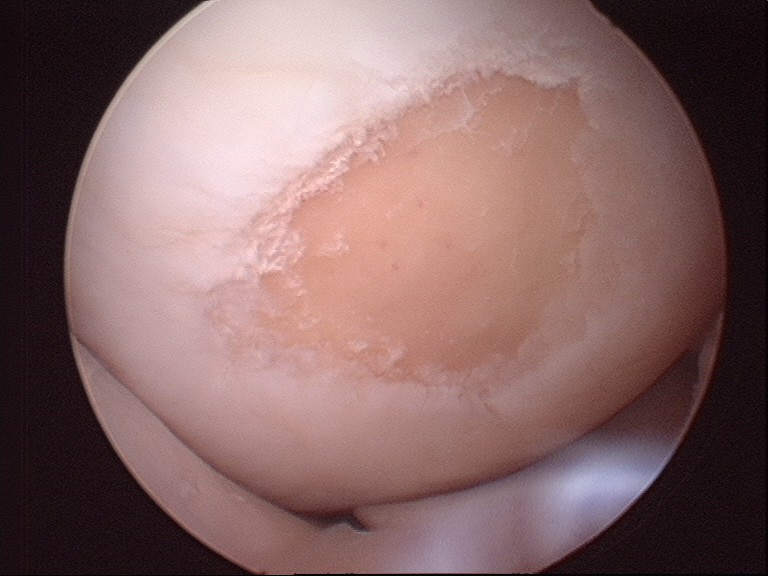
- chondral lesion
-

- chip plantar fetlock joint
-
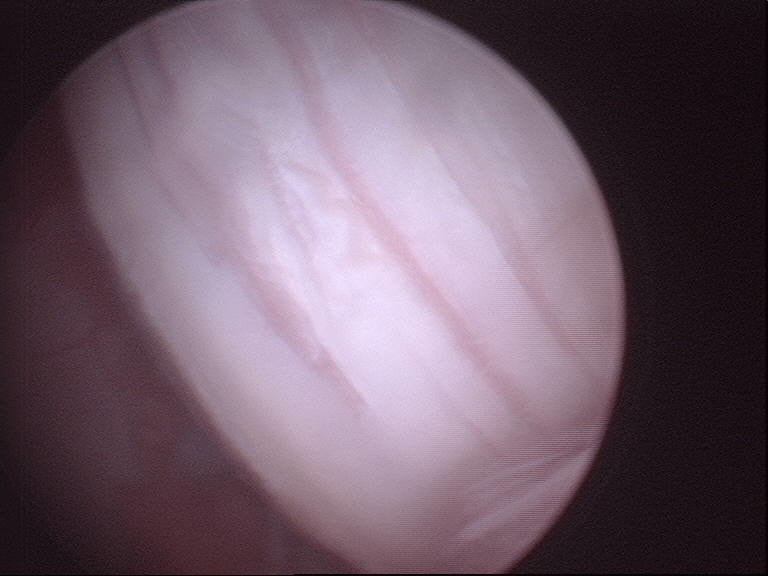
- chondral lesion



